
Quick Answer
Start by mapping telehealth platform payouts as an end-to-end control flow, then enforce a release hold when required evidence is missing. Here, HIPAA context sets privacy boundaries and business-associate expectations, while payout design still needs its own status model, reconciliation trail, and exception handling. Teams should pick architecture only after testing webhook reliability, idempotent retries, and batch failure behavior, then roll out market by market when verification requirements diverge.
Start with scope before architecture#
If you are evaluating telehealth platform payouts, start with one question: can your model still work when privacy obligations, approval controls, and market constraints collide in the same workflow? That matters more than payout anecdotes.
Direct-to-consumer telehealth can look simple at first. Teams hit launch blockers when HIPAA context and payout operations stay on separate tracks until late in the build. Issues surface once provider onboarding, money movement, and patient-linked processes start to overlap.
Use one fixed checkpoint early. Telehealth services provided by covered health care providers and health plans must comply with the HIPAA Rules, and those rules establish standards to protect patients' protected health information. HHS guidance, last updated November 6, 2023, also points to a practical test for remote communication technology vendors: covered providers should use vendors that comply with HIPAA Rules and will enter into a HIPAA business associate agreement.
That does not mean HIPAA defines payout timing, reconciliation, or settlement design. It does mean payout decisions sit inside a privacy and security risk environment that federal guidance explicitly flags for remote telehealth communications. If the boundary between clinical context and payment operations is weak, exposure can increase before your core payout logic is stable.
This article follows a practical path: define scope, map regulatory exposure, compare architecture choices for control and observability, then execute with verification checkpoints. Keep one rule in mind as you read: if your team cannot clearly show where telehealth data handling ends and payout operations begin, pause before adding complexity.
For a Medicare-specific payout walkthrough, see Telehealth Platform Payments: How to Pay Physicians and Specialists Under Medicare Rules.
Define What Telehealth Platform Payouts Actually Include#
Treat telehealth platform payouts as the full flow of moving money to clinicians and partners, not as shorthand for clinician pay anecdotes. Market examples can inform supply thinking, but they do not define how your platform approves, routes, tracks, and closes payments.
Keep planning separated into three layers so decisions do not blur. That makes it easier to see whether a problem is about rates, controls, or operations.
| Layer | What it answers | What to keep in mind |
|---|---|---|
| Rate model | What you pay and why | Many Medicare telehealth flexibilities are authorized through December 31, 2027, and payment parity generally means telehealth is reimbursed at the same rate as in-person care. |
| Compliance model | What must be checked before funds move | Treat compliance requirements and internal controls as a separate design track from pricing assumptions. |
| Operations model | How provider payouts move from approval to final status | Define routing, status states, exception handling, and reconciliation explicitly. |
Do not treat favorable policy context as proof your payout system is ready. Medicare flexibilities are context, not validation of your commercial payer logic, partner contract design, or disbursement workflow. The same caution applies to parity language: in practice, some parity rules act more like price floors and others more like price ceilings, with different economic effects.
Before you expand, use one scale checkpoint: document the full payout flow on one page, from approval trigger to final status. At minimum, name the payee, amount basis, destination account, internal status states, and completion evidence.
State-level snapshots are directional only. State telehealth legislation varies widely, so unsupported anecdotal ranges are not enough for product commitments or legal assumptions.
Payout reliability still affects provider supply. Bad Payouts Are Costing You Supply: How Payout Quality Drives Contractor Retention.
Map the Regulatory Perimeter Before You Build#
Map the perimeter as a decision tool, not as a legal conclusion. For these payout flows, organize review into three internal lanes: data handling, including HIPAA and any EHR-connected touchpoints, financial-controls review, and commercial-conduct review. Then have counsel confirm what is actually required in each launch market.
Build a market-by-market scope matrix#
Use one matrix per market to assign ownership and evidence requirements. Keep it in question form until legal review is complete so open issues stay visible.
| Domain | Before payout release | At final payment status | Audit evidence to retain |
|---|---|---|---|
| HIPAA and EHR-connected data handling | Which payout fields could include patient-linked context? | Which final payment record is needed without pulling clinical payloads into payment logs? | Approved field map, access history, decision record |
| Financial-controls review | What checks are required, if any, and who approves outcomes? | What status proves release, hold, or return? | Check results, timestamps, exception notes |
| Commercial-conduct review | Does this payment need elevated legal review before release? | What documentation supports why it was approved? | Contract/program reference, approval trail, business-purpose record |
Verify legal status before writing policy#
Do not let draft rulemaking quietly become product policy. If HIPAA rulemaking is shaping payout controls, verify status from the official printed PDF artifact, not only the FederalRegister.gov XML rendition. The HIPAA Security Rule cybersecurity entry published on 01/06/2025 (90 FR 898, Document No. 2024-30983, RIN 0945-AA22) is presented as a proposed rule by HHS, not a final rule. FederalRegister.gov also states its XML page is not an official legal edition and does not provide legal or judicial notice.
Treat that check as mandatory before you lock product behavior, customer language, or internal control policy.
Compare Market Entry Reality by Jurisdiction and Care Model#
Compare markets using verified evidence, not implied parity. If two target markets appear to require materially different checks or approval evidence, launch sequentially instead of forcing one universal payout flow.
The current evidence pack supports time-bounded planning signals, including Medicare telehealth flexibilities extended through January 30, 2026 and a stated policy-durability risk. It does not support state-specific claims on payout rails, verification burden, or escalation triggers for Massachusetts, Florida, New York, or Iowa.
| Launch row | Payout rail availability | Verification burden | Regulatory escalation triggers | Known vs unknown |
|---|---|---|---|---|
| Massachusetts | Unknown from current evidence pack. | Unknown from current evidence pack. | Unknown from current evidence pack. | Known: market name is part of the planning set. Unknown: state-specific payout/compliance requirements. |
| Florida | Unknown from current evidence pack. | Unknown from current evidence pack. | Unknown from current evidence pack. | Known: market name is part of the planning set. Unknown: state-specific payout/compliance requirements. |
| New York | Unknown from current evidence pack. | Unknown from current evidence pack. | Unknown from current evidence pack. | Known: market name is part of the planning set. Unknown: state-specific payout/compliance requirements. |
| Iowa | Unknown from current evidence pack. | Unknown from current evidence pack. | Unknown from current evidence pack. | Known: market name is part of the planning set. Unknown: state-specific payout/compliance requirements. |
| Cross-border expansion | Not supported by current evidence pack. | Not supported by current evidence pack. | Not supported by current evidence pack. | Known: tracked as a separate planning row. Unknown: country-specific payout/compliance requirements. |
Use this table as a gating record, not a slide. Keep unknowns visible, assign owners, and require a source artifact before closing each cell.
Then add a second axis for care model so teams do not assume one evidence pattern fits all launch types, because care model changes what you need to verify.
| Care model axis | Key considerations | What remains unknown | Evidence-log action |
|---|---|---|---|
| Synchronous visits | Care model is in scope for launch planning. | Payout cadence and required audit evidence are not specified in the provided excerpts. | Define required payout-state evidence per market before automating release. |
| Asynchronous consults | Care model is in scope for launch planning. | Payout cadence and required audit evidence are not specified in the provided excerpts. | Define required payout-state evidence per market before automating release. |
| Direct-to-consumer telehealth referral patterns | A BMJ Open record documents direct-to-consumer commercial virtual care (2026 Feb 4;16(2):e105555). | The excerpt does not define referral-linked payout structure or compliance checks. | Keep referral-related payouts in a separate review lane until requirements are verified. |
Treat market demand stats as prioritization input, not as payout-control evidence. The ~13-17% visit-share figure can help with market sizing. Control design should rely on verifiable, dated artifacts, for example the September 25-26, 2024 VA SMAG meeting-minutes record, plus market-specific legal and operational confirmation.
Related: Global Payouts and Emerging Markets: 5 Regions Every Platform Should Prioritize.
Choose the Right Architecture for Payout Control and Scale#
Choose for control first, then speed. If finance needs strict reconciliation, audit trails, and defensible exception handling, a ledger-linked design can be safer than one optimized only for the fastest initial integration.
Interoperability alone does not solve payout control. The National Academy of Medicine states that robust interoperability is necessary but not sufficient, and that missing cohesive digital and data architecture can slow innovation and impede care. The same risk shows up here: a payout integration may move money, but you still need auditable states, retries, and references.
| Decision lens | Integrated stack | Standalone payout layer |
|---|---|---|
| Implementation speed | Can be faster when your account model, approvals, and reporting fit the vendor flow with minimal translation. | Depends on how much ledgering, approval logic, and reporting you already own, and may require more explicit mapping before go-live. |
| Control depth | Can be strong when the vendor exposes the hold, release, retry, and reference controls you need; narrower status models can limit control. | Can be strong when you need your own approval logic, ledger states, and market-specific release rules. |
| Observability | Can be good if event logs, payout references, and reconciliation exports are first-class. | Can be good when you maintain raw events plus a canonical internal status layer, with monitoring owned by your team. |
| Vendor lock-in | Can be higher when payout account structure, status language, and reporting semantics are vendor-owned. | Can be lower on orchestration when ledger and references stay internal, though custom abstractions can still create switching cost. |
| Best fit | Early launch where payout rules are simpler and finance can operate from vendor reporting. | Multi-market or higher-control operations where audit, reconciliation, and exception cost matter more than first-release speed. |
Let your operating model decide#
Use one rule: if your team closes books against internal ledger entries, treat vendor statuses as an input, not the only source of truth. Each approval, submission, return, and resolution should map to an internal record that survives retries, disputes, and policy changes.
The CMS LEAD RFA (03/31/2026) reinforces this pattern by separating provisional and final financial settlement, with final settlement listed at page 65. The practical implication is simple: staged settlement states are normal in real financial operations, so collapsing everything into a single "paid" state can create reconciliation risk later.
The tradeoff to state plainly#
Faster integration can raise exception-handling cost later when statuses, retries, and references are not normalized. Early volume can hide this. Scale can expose it through manual reconciliation, support escalations, and ambiguity around payout state.
Checkpoints before you select#
Before you choose, run a failure-path test and keep the results in your selection record. This is where close options usually separate. The LEAD RFA structure also includes screening, application scoring, and explicit risk-control elements, reinforcing the need for clear checkpoints.
| Checkpoint | What to verify |
|---|---|
| Webhook reliability | How failures are surfaced, whether events can be replayed, and how out-of-order delivery is handled. |
| Idempotency behavior | Duplicate submissions and timeout-then-retry flows, including how duplicates are handled in practice. |
| Batch provider payouts under failure | Partial-success batches, item-level status, stable item references, and how failed items are reissued. |
If two options still look close, ask one deciding question: when something fails, can your team prove what happened from internal records without relying on a single vendor screen?
If architecture choice is the sticking point, compare Integrated Payouts vs. Standalone Payouts: Which Architecture Is Right for Your Platform?.
Design Minimum Viable Compliance Gates and Evidence#
Set the hold rule before you scale telehealth-adjacent workflows: if a required compliance artifact is missing at decision time, hold the action and route it to manual review. A practical baseline is clear ePHI labeling in flow, in-context consent/privacy disclosure, documented data-use and retention intent, and strong access controls for sensitive features.
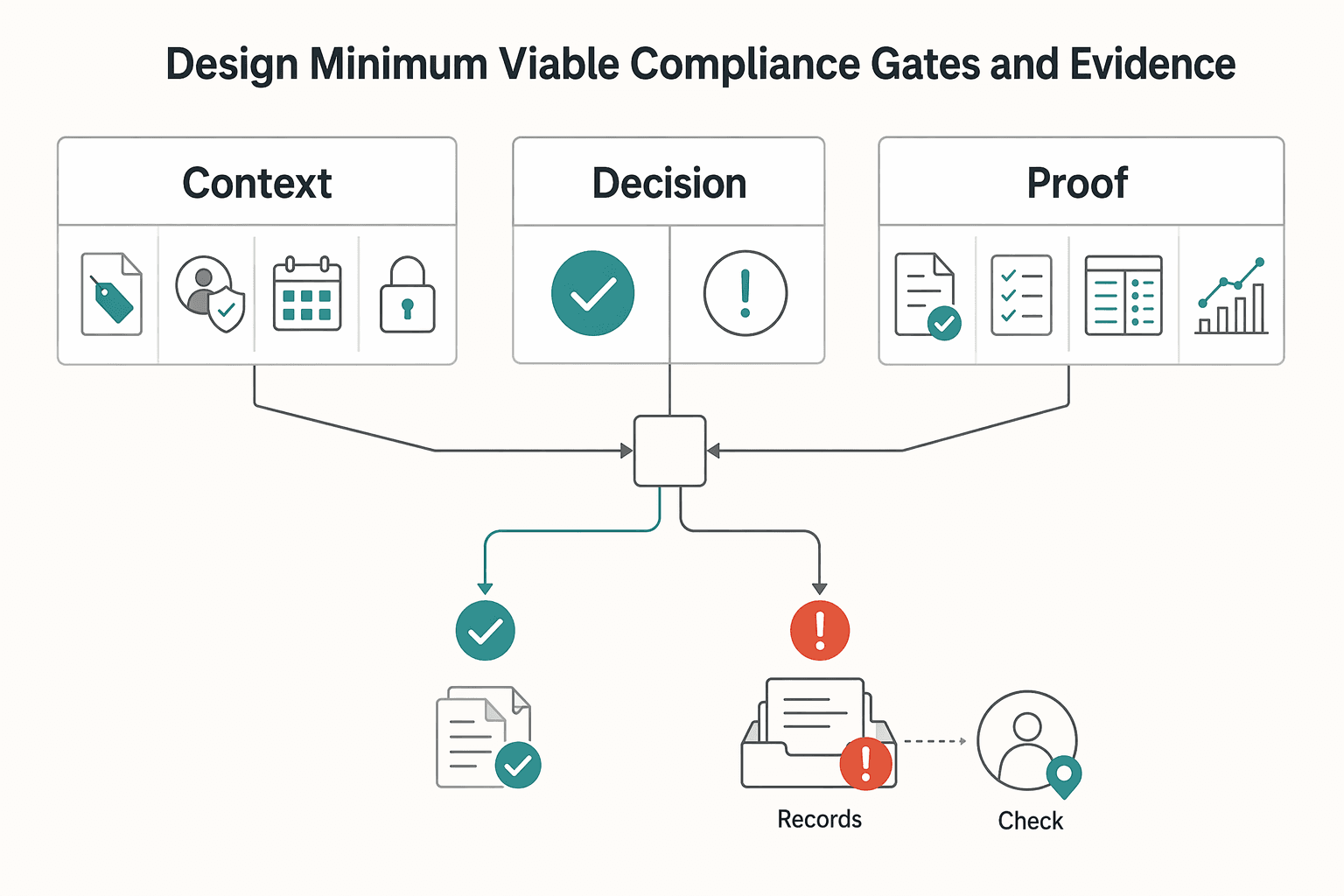
Post-hoc cleanup is where control breaks down. If a step proceeds before the record is complete, teams end up reconstructing intent after the fact. The safer pattern is simple: make the decision provable from your own records before submission.
Minimum gates worth enforcing#
These are the gates worth making explicit in product and ops. They should be visible in the workflow, not buried in policy text.
| Gate | Workflow requirement |
|---|---|
| ePHI visibility gate | Clearly indicate when ePHI is being collected or displayed. |
| Consent/privacy gate | Present consent and privacy notices in context, not as long legal blocks. |
| Sensitive-feature access gate | Gate sensitive portal pathways with multi-factor authentication. |
| Data-security gate | Avoid known TMIS failure modes by preventing unencrypted medical-data storage and requiring authentication controls that include message authentication. |
More controlled access can slow timeliness and increase administrative work, but that tradeoff can be necessary for stronger control coverage.
What the evidence pack should contain#
Each workflow decision should produce a compact evidence pack that can stand on its own. At minimum, include the items below and keep them tied to the same record.
- where ePHI was collected or displayed in the flow
- the in-context consent/privacy notice shown at the decision point
- why data was requested, how it is used, and how long it is retained
- access-control and authentication status for sensitive features (including MFA)
Use a recurring check: sample completed records and confirm ops can reconstruct the decision from the record alone. Track operational checkpoints such as portal activation, appointment completion, and task success rates.
Keep HIPAA-adjacent risk bounded#
Keep TMIS and portal data handling tightly scoped. If ePHI is collected or displayed in any flow, label that clearly and keep it out of records that do not require it.
Write the boundary down: which screens, exports, and attachments may contain ePHI, and which may not. Gate sensitive portal features with multi-factor authentication, and avoid authentication paths that make decision trails hard to trust.
For a provider-side comparison with similar HIPAA constraints, see Mental Health Platform Payments: How to Pay Therapists and Counselors in Compliance with HIPAA.
Build the Money Movement Sequence Operators Can Audit#
For payout flows, treat money movement as an ordered decision chain, not as a single release action. If your team cannot show where a payment sits between its trigger and final reconciliation, operators will struggle to audit what happened.
That follows a basic audit pattern in healthcare billing: each decision affects the next, and skipped steps create blind spots. Earlier control decisions determine what can happen downstream. This section is about proving the full sequence later from your own records.
Put the sequence in writing#
Write one upstream-to-downstream order and keep it consistent. Define clear stages from the originating record through payment release and reconciliation closure.
The key is not the label set. The key is the trace. Each stage should be distinguishable, with enough detail to show what happened and why, without rebuilding the timeline from email or vendor dashboards. Do not collapse multiple stages into one status just to simplify UI copy.
Use platform features that reduce ambiguity#
Retries, event updates, and balance views can serve as practical controls, not healthcare mandates. Use them so engineering and finance can work from one source of truth.
Each initiation should carry a stable internal payout identifier so retries do not create ambiguity. Keep status history and reconciliation anchored to your internal ledger and state. If records disagree, treat it as an exception before closure.
Add handoff checkpoints with clear ownership#
Every handoff needs an explicit confirmation point and owner. Use checkpoint names that fit your stack, but keep the chain complete from initiation through final resolution.
If policy-based screening or risk controls apply, record that decision in the same trail. For each checkpoint, store who or what created it, when it happened, and which prior state it depended on. Manual fixes in chat or tickets should be written back into the payout record, or the audit trail breaks.
Keep care workflows and payout controls on separate tracks#
Keep a clear internal boundary between care-delivery workflows and money-movement controls. This is a control design choice, not a claim that one model is legally required.
That boundary matters even more in cloud environments, where responsibilities vary by service model and provider agreement. Route money-movement decisions through one defined control path so decision and resolution evidence stays auditable.
Related reading: What Is a Demand-Side Platform (DSP)? How Programmatic Ad Platforms Manage Publisher Payouts.
Handle Failure Modes Before They Become Brand Risk#
Treat failure handling as a defined control path, not as an ad hoc ops response. When records stop making sense, your team should already know how to classify, contain, and resolve the issue.
A practical way to structure this is Failure Mode and Effects Analysis, or FMEA: name the failure mode, likely cause, effect, and mitigation before incidents pile up. In one telehealth FMEA, an eight-member multidisciplinary team prioritized risk using severity, probability, and detectability scores, or RPNs. The same discipline is useful here, especially because telehealth safety data are still limited.
Focus first on ambiguous operational exceptions#
Start with the cases that create disagreement between system state and operator interpretation. In the telehealth FMEA, risk drivers included obsolescence, economic issues, and technology literacy.
For each case, define in advance the detection signal, owner, immediate containment action, and closure evidence.
Route incidents by severity#
Use a simple escalation path your team can follow under pressure. Keep it written down and easy to find.
- Process or transport disruptions: controlled retry or restart path.
- Compliance or screening flags: manual review with a documented decision trail.
- Legal or regulatory interpretation questions: legal escalation.
If a legal or regulatory interpretation is based on FederalRegister.gov XML text, verify it against an official Federal Register edition before treating it as authoritative.
If records diverge, contain first, reconcile second#
If key records diverge, apply a documented containment rule before further processing, then reconcile to restore internal consistency.
Keep incident evidence in the control trail so resolution is auditable from one source of truth.
The broader payout-control model is laid out in Gruv Platform Payments for Global B2B Payouts and Compliance.
Set Provider Payout Policy Without Overpromising Rates#
Set payout policy around controls you can enforce, not around anecdotal rate expectations across markets.
Keep the split explicit: rates are a contracting decision, while payout policy is a payment-integrity decision. You can promise process with confidence, but not outcomes you do not control. In practice, use conditional payout language tied to required checks, and state that timing can vary when review requirements are not yet met. If release depends on documentation review, pricing validation, or manual review, avoid absolute wording.
Your strongest policy anchor is the prepayment checkpoint. Before release, confirm documentation is complete, required coding details are present, and the payment amount matches the contractually agreed price. That maps policy to enforceable controls and gives you a valid delay reason when documentation or coding issues would otherwise lead to recoupments, denials, or legal issues. If you depend on post-payment correction, expect more provider and payer friction and administrative burden. Avoid promising a consistently smooth experience.
Provider onboarding template#
Use language your ops team can point to during payout questions. It should map cleanly to the controls you actually run.
- What we confirm before payout: We confirm required supporting documentation has been received, required coding details are present, the payment record passes our prepayment review, and the amount matches the applicable contract terms.
- What may delay payout: Payout may be delayed if documentation is incomplete, coding details need correction, payment terms cannot be matched to the underlying agreement, or the record requires manual review.
Before go-live, treat any policy statement that cannot be traced to a product control, review step, or evidence artifact as a rewrite requirement. In disjointed systems, that gap widens quickly.
Use a First 90-Day Execution Checklist#
Once policy and control design are set, turn them into a dated launch plan. Use a 13-week checklist only as an internal template, not as an evidence-backed telehealth payout standard. The excerpts support planning rigor (dated records, section-level artifacts, and security cautions), but they do not validate a required week-by-week rollout sequence.
| Timing | Focus | Key actions |
|---|---|---|
| Week 1 to 2 | Initial scope and owners | Define initial scope, assign owners for each control point, record what triggers review, and note where decision evidence is stored. |
| Week 3 to 6 | Evidence-log format | Record dated checkpoints, separate event dates from report or review dates, capture concrete section artifacts, and log compliance-style checkboxes explicitly. |
| Week 7 to 10 | Internal evidence-quality review | Mark which items are supported by official-source excerpts, identify which are still assumptions, and state uncertainty directly where execution specifics are still unknown. |
| Week 11 to 13 | Written, dated readiness review | Complete a written, dated readiness review with explicit gaps and deferrals, and defer if ownership, evidence handling, or exception paths are unresolved. |
Week 1 to 2#
Define initial scope and assign owners for each control point in that scope. For each control, record who owns it, what triggers review, and where decision evidence is stored. Keep sensitive information in official, secure systems rather than ad hoc channels.
Week 3 to 6#
Build the evidence-log format you will use throughout the launch. Record dated checkpoints, separate event dates from report or review dates, and capture concrete section artifacts for material decisions. If you use compliance-style checkboxes, log them explicitly so reviewers can trace what was affirmed.
Week 7 to 10#
Run an internal evidence-quality review before expanding scope. Mark which items are supported by official-source excerpts and which are still assumptions, and avoid treating database inclusion alone as endorsement. Where execution specifics are still unknown, state that uncertainty directly.
Week 11 to 13#
Complete a written, dated readiness review with explicit gaps and deferrals. Treat this timing window as internal governance, not a source-validated launch standard. If ownership, evidence handling, or exception paths are unresolved, defer and launch sequentially.
If your checklist is set, map each control point to concrete API and webhook states. That lets ops and finance verify every handoff in one workflow: Review Gruv docs.
Conclusion#
Strong teams do not start with pay-rate chatter. They start with a compliance-scoped, auditable payout design that still holds up when you add a new market, care model, or reimbursement path.
That approach is practical because telemedicine payments are often not generic checkout flows. Processing may need healthcare-specific compliance handling, security controls like encryption and fraud prevention are central, and onboarding has to stay fast while still meeting regulatory standards.
Before you choose architecture or set a launch date, build two artifacts: a market comparison table and a minimum control checklist. In the table, compare each target market and program by care model, payout dependencies, verification burden, and unresolved unknowns. In the checklist, define the minimum evidence required before funds move, who can approve exceptions, and what triggers a hold instead of release.
Keep the first pass exact. For subscription models, confirm onboarding actually establishes reliable automated billing. For marketplace models, include provider-level risk review, since mixed provider risk profiles can complicate onboarding and approval decisions. If those checks are not explicit in writing, rollout is still being driven by assumptions.
Demand signals are useful, but they are not launch criteria. Directional estimates suggest telehealth moved from a small share of outpatient visits before COVID to a sustained minority share in 2023-2024, yet growth does not replace traceable controls. Confirm market and program coverage, then lock your control requirements before committing engineering and go-to-market spend.
Before you lock launch dates, confirm market coverage, payout rail options, and policy-gate requirements for your exact program: Talk with Gruv.
Frequently Asked Questions
What does "telehealth platform payouts" include beyond clinician pay rates?
It includes the full payout operation, not just the amount paid: release criteria, status tracking, reconciliation, and payment evidence. In telehealth, payout design is tied to reimbursement logic, so billing prerequisites matter before money moves. For example, listed Medicare RPM references include CPT codes 99091, 99453, 99454, 99457, and 99458, and the cited billing artifact is a 1500 form with the supervising QHCP NPI.
Which compliance layers should be implemented first for HIPAA-context provider payouts?
There is no single universal order that fits every telehealth model or market. Start by defining scope, data boundaries, and the minimum evidence required before a payout is released, then build hold paths for missing artifacts. If you are operating in reimbursement programs, include the required program prerequisites and documentation steps up front rather than after launch.
How is pharma-to-telehealth commercial payment risk different from routine provider payout operations?
Do not treat pharma-linked payments as routine provider disbursements by default; route them through separate legal and compliance review before release.
How should founders treat pay-rate anecdotes from Reddit or Facebook when planning expansion?
Treat them as weak signal, not as decision-grade evidence. Telehealth reimbursement rules differ across Medicaid, Medicare, and private insurance, with federal and state oversight layers. Before expanding, verify plan-level CPT, credentialing, and prior-authorization requirements rather than relying on social posts.
What should a telehealth team compare when choosing a telehealth payouts API?
Prioritize operational control and traceability over feature checklists. Compare how clearly the system supports payout evidence, status history, and reconciliation when exceptions occur. Specifically test holds, returns, retries, and duplicate scenarios before treating the flow as production-ready.
Which signs suggest a payout flow is not audit-ready yet?
A payout flow is not audit-ready if you cannot produce consistent evidence for why a payment was released and how its status changed. It is also not ready when provider-facing payout states do not line up with finance reconciliation outputs. Missing dated records for exceptions and sign-offs is another clear warning sign.
When should a platform pause rollout in a new state or country?
Pause when the new market requires checks your current flow does not yet implement or validate. Pause again when policy assumptions are stale, because telehealth policy drift can translate into denied claims and downstream payout issues. If you cannot verify plan-level eligibility and billing prerequisites, run sequentially instead of forcing one rollout pattern everywhere.
Try a related tool
Researched and edited by the Gruv editorial team. Gruv builds cross-border billing, payouts, and finance-operations software for global businesses.
Sources
- cms.gov/priorities/innovation/files/lead-rfa.pdftrusted
- department.va.gov/privacy/wp-content/uploads/sites/5/2026/04/F...trusted
- department.va.gov/advisory-committee-management/wp-content/upl...trusted
- fcc.gov/covid-19-telehealth-program-frequently-asked...trusted
- federalregister.gov/documents/2025/01/06/2024-30983/hipaa-securi...trusted
- federalregister.gov/documents/2024/01/09/2023-28857/health-data-...trusted
- govinfo.gov/content/pkg/CHRG-114shrg69104673/html/CHRG-1...trusted
- hhs.gov/hipaa/for-professionals/privacy/guidance/res...trusted
Educational content only. Not legal, tax, or financial advice.
Related Posts

Integrated Payouts vs Standalone Payouts for Platform Architecture Decisions
**Treat integrated and standalone payouts as an architecture decision, not a product toggle.** The real split is the same one you see in payment processing more broadly: either payments are connected to the core platform experience, or they are not. [Lightspeed](https://www.lightspeedhq.com/blog/payment-processing-integrated-vs-non-integrated) puts that plainly in POS terms: your payment terminal either speaks to your point of sale, or it does not. For platform teams, the equivalent question is whether payment flows run through one connected system or sit in separate lanes you manage independently.

How Platforms Should Prioritize 5 Emerging-Market Payout Regions
If you are choosing where to launch cross-border payouts in 2026, start with what your team can actually run. Too many "top" lists lean on hype or market-cap tables. That may work for headlines, but it does not help with execution.

Bad Payouts Are Costing Your Supply in Two-Sided Platforms
Payout issues are not just an accounts payable cleanup task if you run a two-sided marketplace. They shape supply-side trust, repeat participation, and fill reliability. They can also blur the revenue and margin signals teams rely on.