
Quick Answer
Choose a payout model only after proving it can handle rate swings, cancellations, and classification scrutiny in live operations. For shift-based pay gig healthcare workers, the practical winner is the model that keeps every accepted shift auditable, keeps onboarding verifiable, and keeps disputes resolvable without margin surprises. Evidence in the article points to a real tradeoff: fast fill can improve speed, but weak controls can raise legal and safety risk.
Execution Risk in Shift-Based Healthcare Pay Goes Beyond Posted Rates#
The headline story around shift-based pay for gig healthcare workers is usually built on snapshots: a surge-priced shift, a fast fill, a worker who likes the flexibility. That is not enough to make an operating decision. The real question is whether your payout model still works when rates move with demand, work is booked shift by shift, and facilities change or cancel needs with very little notice.
That tension is already visible in the market. The Roosevelt Institute describes on-demand nursing companies such as CareRev, Clipboard Health, ShiftKey, and ShiftMed as promising hospitals more control and nurses more flexibility. At the same time, its reporting from 29 interviews with gig nurses and nursing assistants points to schedule uncertainty and weak accountability for worker safety. The Markup also notes that app-based healthcare shifts are booked as individual blocks of hours, with rates that can rise when demand rises. For founders, variable payouts are not just a pricing feature. They can shape trust, retention, exception handling, and facility confidence. Three decision lenses matter from the start:
- Payout volatility
Variable shift rates are often used when facilities need urgent coverage, especially when a unit is short staffed. The real differentiator is not whether you can raise rates. It is whether you can explain, track, and reconcile those changes without confusing workers or blowing up unit economics.
- Scheduling reality
In this model, workers often book one shift at a time rather than on a long scheduling horizon. The important question is how your operation handles uncertainty, because cancellation risk and short-notice changes can quickly turn an attractive posted rate into a poor worker experience.
- Evidence quality
Vendor claims about flexibility are easy to find. The useful standard is whether you can support launch decisions with evidence that reflects real operating conditions, such as the Roosevelt Institute interview findings or firsthand reporting like the March 31, 2025 STAT piece describing workers waking up early to see whether a shift was canceled.
This guide stays focused on variable contractor payouts for on-demand nursing platforms and the places they get harder to manage as you scale. You will not get a universal winner here, because the evidence does not support one. You will get a practical way to judge which model can hold up under margin pressure and facility-level volatility.
If you are evaluating this category, verify three things before you get excited by fill-rate anecdotes. Check how rates change, what happens when a booked shift is canceled, and whether every payout can be traced back to a specific accepted shift. If you cannot answer those cleanly, you do not have a scalable model yet.
Who this guide is for and how to choose a payout model#
This guide is for founders and marketplace operators comparing payout models used by CareRev, ShiftKey, ShiftMed, and Gig Healthcare. Before launch, screen each model through four filters: payout volatility tolerance, 1099 classification exposure, facility mix, and evidence quality. If your team cannot monitor both worker outcomes and facility risk, pause a variable-rate launch.
| Filter | What to check | Grounded detail |
|---|---|---|
| Payout volatility tolerance | Decide how much rate movement your margins can absorb before filled shifts become a finance risk | Require traceable payout records for each accepted shift; if pricing swings are doing most of the fill work, treat that as an operating warning sign |
| Legal exposure under 1099 contractor classification | Treat classification as a core operating constraint, not a legal footnote | The IRS groups worker-classification evidence into behavioral control, financial control, and relationship of the parties; DOL 2024 final rule guidance took effect on March 11, 2024 |
| Facility mix | Match your payout model to care setting realities | CareRev publicly frames its model around hospitals; ShiftKey markets to Skilled Nursing Facility (SNF) operators and reports 6,000+ facilities on platform use for PRN shifts (vendor claim) |
| Evidence quality | Use verifiable operating evidence, not marketing claims alone | Exclude markets where you cannot verify onboarding, safety readiness, and payout traceability |
- Payout volatility tolerance
Decide how much rate movement your margins can absorb before filled shifts become a finance risk. Require traceable payout records for each accepted shift so disputes and reconciliation can be handled cleanly. If pricing swings are doing most of the fill work, treat that as an operating warning sign.
- Legal exposure under 1099 contractor classification
Treat classification as a core operating constraint, not a legal footnote. The IRS groups worker-classification evidence into three categories: behavioral control, financial control, and relationship of the parties. The DOL also describes misclassification as a serious problem, and its 2024 final rule guidance took effect on March 11, 2024.
- Facility mix
Match your payout model to care setting realities. CareRev publicly frames its model around hospitals, while ShiftKey markets to Skilled Nursing Facility (SNF) operators and reports 6,000+ facilities on platform use for PRN shifts (vendor claim). Hospital and SNF environments can create different onboarding, training, and risk pressures.
- Evidence quality
Use verifiable operating evidence, not marketing claims alone. Roosevelt Institute warns that nurses may be placed in unfamiliar environments with no onboarding or facility training, so exclude markets where you cannot verify onboarding, safety readiness, and payout traceability. Claimed credential verification and hour tracking are useful signals, but they are not proof of controlled outcomes by themselves.
Related: Bitcoin and Ethereum Payouts for Gig Workers: Tax Reporting and Volatility Management.
Quick comparison of payout models for on-demand nursing platforms#
Choose your payout model by control exposure, not brand. Here, the most reliable comparisons come from clearly labeled vendor claims, one policy brief, and one media anecdote, with visible unknowns.
Independent evidence is limited: the Roosevelt Institute brief draws from 29 interviews, and the Business Insider piece reflects 3 nurses. Use both to spot risk patterns, not to make market-wide conclusions.
| Example | Model type | Best for | Margin behavior under surge demand | 1099 contractor classification risk | Operational complexity | Known vs unknown |
|---|---|---|---|---|---|---|
| CareRev [vendor claim] | Dynamic-rate marketplace with a facility-set base rate and platform recommendations | Teams that want variable pricing with defined bounds | CareRev says Smart Rates adjusts around base rate at -10%, 0%, +10%; this is the clearest public bound in this set | Material if contractor labeling conflicts with real control over work acceptance and performance | Medium to high | Known: dynamic-rate tooling and disclosed adjustment band. Unknown: independent facility-level outcomes for credentialing, safety readiness, and dispute results |
| ShiftKey [vendor claim] | Criteria-based dispatch with Instant Accept auto-approval | Fast-fill operations with lower manual approval friction | Auto-approval may improve fill speed; no public surge-band cap is provided here | Can increase if criteria and downstream rules reduce worker independence | Medium to high | Known: Instant Accept exists. Unknown: independent evidence on payout disputes, readiness in unfamiliar settings, and margin stability |
| ShiftMed [vendor claim] | Compliance-forward staffing posture | Operators prioritizing audit and compliance posture | Confirm public rate-band mechanism with the platform directly | Misclassification is explicitly framed by ShiftMed as a serious penalty/audit risk | High | Known: misclassification risk is explicitly highlighted. Unknown: payout-band detail, dispute-flow detail, and independent market-by-market evidence |
| Clipboard Health [vendor claim + media anecdote] | Flexibility-first facility-professional matching marketplace | Broad matching and worker flexibility positioning | No public rate-band detail here, so surge behavior is harder to model | Material if independence positioning is not matched by common-law independence evidence | Medium | Known: platform positions itself as connecting independent professionals and facilities. Unknown: pricing controls, audit-trail strength, and safety consistency; BI's 3-nurse lens is directional only |
| Gig Healthcare [vendor claim] | Multi-segment offering: travel, per diem, and permanent opportunities | Teams serving mixed demand types | Harder to model as one shift-pricing system across mixed engagement types | Varies by engagement type; no single status assumption should be made | High | Known: public positioning across travel, per diem, and permanent opportunities. Unknown: segment-level contractor posture, rate-setting logic, and dispute evidence |
| Checkpoint before market entry [operator requirement] | Launch gate, not a brand model | Any new facility segment or geography | Do not launch unless each accepted shift maps to worked time, payout calculation, and reconciliation | Contractor labels alone are insufficient; IRS treatment follows common-law control/independence evidence | High upfront | Must be true: verified credentialing quality, documented payout controls, owned dispute path with timing, and exportable audit trail |
Two practical readouts stand out. First, CareRev is the only example here with a publicly stated adjustment band, so it offers a concrete pricing-control signal rather than flexibility language alone. Second, faster assignment logic like Instant Accept can reduce booking friction, but readiness, time, or rate issues can still surface after the work is done.
The Roosevelt and Business Insider evidence gaps are the main confidence constraint. Roosevelt describes algorithmic management entering healthcare labor markets and flags uncertainty and safety concerns from its 29-interview sample; Business Insider provides useful experience detail from 3 nurses, but not broad generalization. At facility level, one operator reported relief and said gig workforce pay rates were 10% to 20% lower than agency nurses: "This does provide a relief." Treat that as anecdotal signal, not universal proof.
Marketplace contractor model with variable shift multipliers#
Use this model when your priority is fast fill in fragmented markets, and only if you run payout logic and contractor-classification evidence as core operations, not app UX.
- Best fit: fragmented geographies with uneven shift supply, including patterns like app-led dispatch seen in rural Pennsylvania.
- Main upside: faster liquidity from flexible shift acceptance, demand-responsive rates, and request flows that can be manual or auto-accepted.
- Main risk: trust and compliance pressure increase when pay varies without clear allocation logic and the worker is labeled as a contractor while control signals rise.
- Pilot posture: launch in one metro, keep surge behavior policy-bounded, and require post-shift reconciliation before multi-facility expansion.
Variable pricing can help clear urgent coverage gaps because facilities can raise rates under demand pressure and workers can adjust bids in at least some documented flows. The speed benefit is real, but so is the governance load.
Trust usually weakens when workers cannot see how shifts are allocated or why same-place, same-time work pays differently. Classification scrutiny also rose after the U.S. Department of Labor's final rule published on January 10, 2024 (effective March 11, 2024), with explicit warning that misclassification can deny wage-and-hour protections.
Run this model with a per-shift evidence trail: request timestamp, acceptance path (manual or auto), credential status, worked-time record, payout calculation, and any adjustment or dispute outcome. If acceptance rises while repeat-shift behavior falls in your own data, treat it as a warning to tighten matching, facility criteria, and onboarding before scaling worker volume.
Contractor payouts also add reporting and money-flow complexity. ShiftKey's FAQ describes a three-party 1099-K structure and cites a 2025 threshold of more than $20,000 and over 200 payments, so your records need to support traceability even if that threshold is not your primary launch decision.
Managed staffing model with tighter compliance controls#
If your priority is a staffing model a hospital compliance team can defend, managed staffing is usually the safer operating posture than a loose contractor marketplace. It usually scales more slowly because tighter controls add operational overhead. The tradeoff is stronger evidence on worker status, credentialing, and facility readiness.
- Employer-led staffing posture
This model works when your day-to-day controls match an employer-led setup. ShiftMed describes its approach as a local on-demand W-2 healthcare staffing model and says the employer of record takes on payroll taxes, benefits, and workers' compensation. That framing matters because IRS common-law rules still determine worker status, and the U.S. Department of Labor rule currently in effect took effect on March 11, 2024.
The practical test is not brand language. It is whether classification matches how work is actually directed. If your legal posture depends on 1099 labels but operations are tightly controlled, treat that as a review point before scaling.
- Credentialing evidence you can produce on demand
Managed staffing is strongest when each shift has a complete, auditable clinician file. NAMSS defines credentialing as obtaining, verifying, and assessing practitioner qualifications to provide patient-care services. In practice, your pre-shift record should show verified license or certification status, role match, required facility training, and clearance for that care setting before assignment.
One health-system app example says nurses are thoroughly vetted for required licenses, certifications, and training alignment. That is the operating standard to replicate. The failure pattern is also clear: placement into unfamiliar clinical environments without onboarding or facility training, plus weak accountability for worker safety.
- Where tighter controls pay off operationally
This approach fits hospital and Skilled Nursing Facility (SNF) partners that require stronger controls before approving recurring shift pools. One reported health-system program planned to expand gig staffing to 19 hospitals and nursing homes from 12, which shows controlled app-based staffing can extend across facility types when onboarding and vetting are disciplined.
Keep rollout criteria explicit: do not launch a recurring pool until each facility owner signs off on orientation responsibility, accepted roles, and credential-review timing. A clear red flag is recurring-demand requests without documented unit-specific training ownership or escalation paths when issues occur. For operators in this category, that documentation is what makes each placement defensible.
Hybrid model by facility segment and role type#
A hybrid model works when you split staffing rules by facility segment and role risk instead of forcing one payout and control model across every shift.
- Hospitals and higher-acuity placements
Keep these in a controlled track. Mixed-facility expansion is real, but the reported Providence expansion from 12 to 19 hospitals and nursing homes points to segment-specific operating rules, not one generic marketplace flow. In practice, this is the lane where fixed payout bands and tighter release criteria are usually easier to defend.
- Skilled Nursing Facility (SNF) coverage
Use SNFs as a middle lane with clear boundaries. App-based matching is already used across hospitals and healthcare facilities, including firms such as CareRev, Clipboard Health, ShiftKey, and ShiftMed. Define in writing which SNF roles stay managed and which can enter a limited-flex pool, then apply that rule consistently.
- Lower-risk overflow and app-led contractor pools
Put flexible, demand-sensitive pricing here. App-enabled contractor staffing is already used by health systems, and rates can increase with demand, so surge logic belongs in this lane if you use it. Set surge-eligible roles before launch and keep payout guardrails explicit.
The tradeoff is policy complexity, especially around 1099 contractor classification. Under the FLSA framework, there is no single rule for contractor status, and the economic reality analysis uses six factors. If your controlled and flexible lanes become operationally identical, your product may look hybrid while your classification posture does not.
Before GTM rollout, publish a role-by-facility matrix that names worker status, pricing mode, onboarding owner, and required pre-shift documentation. Use it as a hard checkpoint when demand spikes so hard-to-fill shifts do not silently bypass the stricter lane.
Related reading: German Blue Card for Highly Skilled Workers: Eligibility, Net Pay, Tax, and Freelance Tradeoffs.
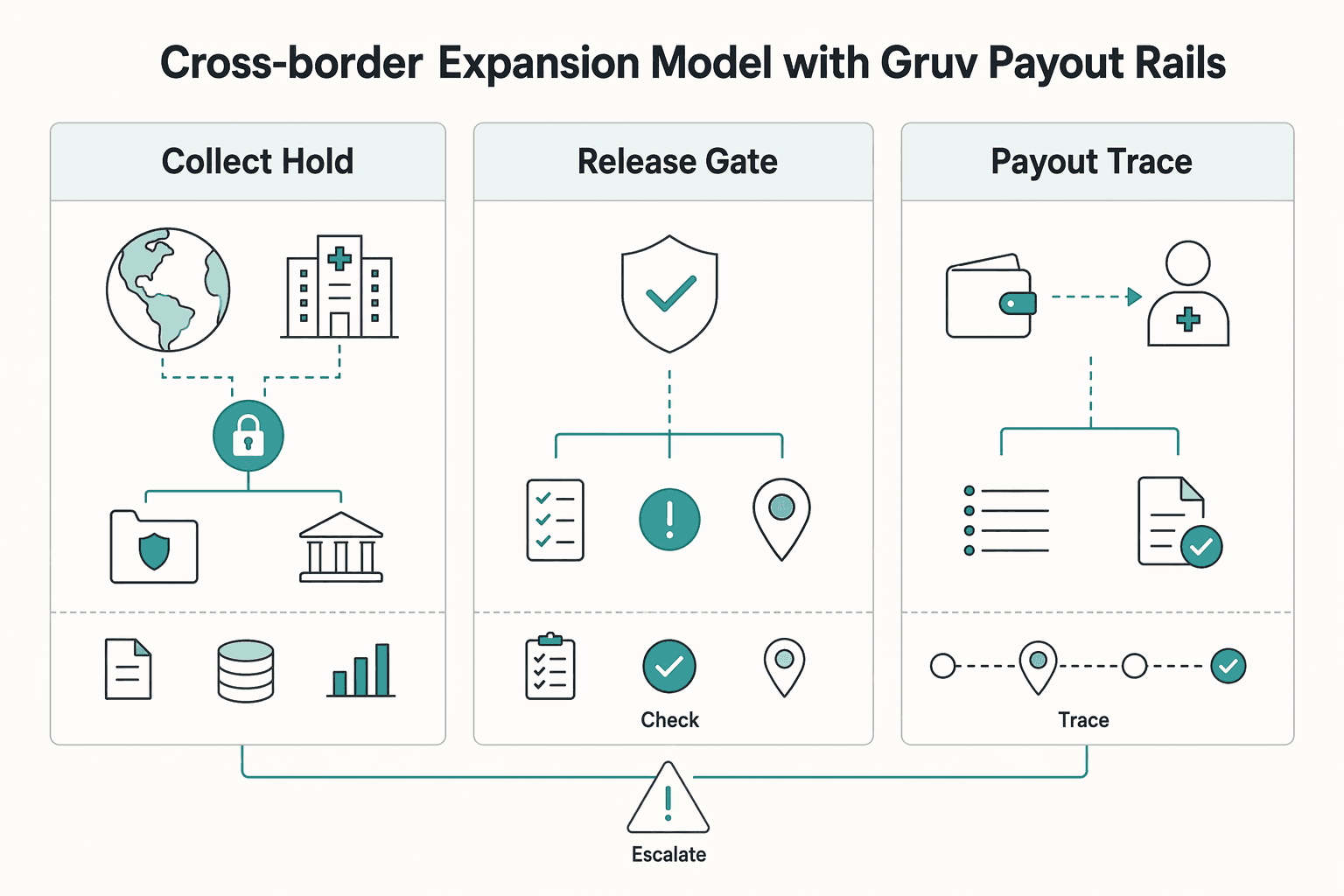
Cross-border expansion model with Gruv payout rails#
Cross-border expansion works when payout operations follow a strict order: collect, hold, check, pay, then reconcile, with country controls enabled before volume scales.
| Stage | Required control | Grounded detail |
|---|---|---|
| Collect and hold funds before payout release | Use a collect-then-disburse flow with a holding step, not direct pass-through | Unsupported cross-border flows return errors; one documented supported set includes the United States, Canada, United Kingdom, EEA, and Switzerland |
| Gate onboarding by market, before first payout | Collect KYC/KYB onboarding data upfront where required and route tax intake by payee type | Individuals use Form W-8BEN; entities use Form W-8BEN-E; these forms go to the payer or withholding agent, not directly to the IRS |
| Make payout execution idempotent and reconcile from the ledger | Link each shift, charge, transfer, and payout attempt | Monitor payout lifecycle states such as paid, failed, and canceled; expand to additional countries only after duplicate-prevention tests pass |
- Collect and hold funds before payout release
Use a collect-then-disburse flow with a holding step, not direct pass-through. A documented payout-rail pattern supports funds segregation, so funds from separate charges and transfers can be held on the platform before transfer to recipients. That creates a real policy gate between facility payment and worker payout.
Corridor limits are the first operational constraint: unsupported cross-border flows return errors. One documented supported set includes the United States, Canada, United Kingdom, EEA, and Switzerland. Keep a pre-launch country matrix for origin country, recipient country, worker type, and support status before shifts go live.
- Gate onboarding by market, before first payout
Treat compliance as an entry condition, not a cleanup step. Where required, collect KYC/KYB onboarding data upfront and pass it through before workers start taking shifts. Tax intake also needs payee-type routing: individuals use Form W-8BEN, entities use Form W-8BEN-E, and these forms go to the payer or withholding agent, not directly to the IRS.
Keep this market-specific instead of copying one domestic onboarding flow into every market, including domestic pilot patterns like CareRev or ShiftMed. Store a clear evidence pack per payee and review tax-form freshness during onboarding audits.
- Make payout execution idempotent and reconcile from the ledger
Variable shift payouts must be retry-safe. Idempotent requests are the control that prevents duplicate payout side effects when retries happen after timeouts or transient failures.
Run ledger-first reconciliation by linking each shift, charge, transfer, and payout attempt, then monitor payout lifecycle states such as paid, failed, and canceled. If your rail supports automatic payouts that preserve transaction-to-payout association, use it to reduce reconciliation overhead. Expand to additional countries only after duplicate-prevention tests pass and payout exceptions can be explained from ledger records.
For a step-by-step walkthrough, see Best Way for a German Agency to Pay a US-Based Freelancer.
Red flags that kill margin and create legal exposure#
If any of these signals show up in your market, treat them as a pause condition, not a minor optimization.
- Headline proof instead of launch proof
Media recognition and polished marketing can show category momentum, but they are not launch evidence for safety controls, legal defensibility, or unit economics. Use your own operating evidence instead: credential completion, payout exception logs, cancellation patterns, repeat-shift behavior, and a documented dispute path by facility.
- Supply that only holds when surge pricing stays on
If your supply clears only when rates stay elevated, margin is likely fragile. Reporting notes that facility-offered rates can rise with demand, and hospitals are already under pressure from contract-labor costs, so permanent surge dependency is easy for buyers to cut. Check baseline fill, day-of cancellation, and repeat-shift behavior before expansion.
- Thin onboarding at unfamiliar facilities
Thin onboarding in unfamiliar facilities is both a legal and safety risk. Interview-backed reporting flagged placements with no onboarding or facility training, and nurse testimony also reflects unstable shift reliability: "It's a gamble. ... I'll wake up at 5 in the morning, and I'll find out if I'm canceled or not." If you cannot show orientation completion, role expectations, unit contact, and escalation paths before first shift, quality risk rises while contractor-classification exposure remains harder to defend.
What to decide before you commit engineering and GTM budget#
Commit budget only after one operating model passes a live market test on compliance, onboarding, and payout controls, not just headline shift rates.
- Choose the model that matches your risk tolerance and control reality
Start with control and independence, not pricing anecdotes. If facilities need employer-like control over schedules, conduct, and work methods while the model depends on contractor flexibility, treat that as a classification risk under the IRS control-and-independence standard. Keep this as an active gate: the U.S. Department of Labor published its final rule on January 10, 2024, effective March 11, 2024, and also points to 2026 misclassification rulemaking context.
- Require a market-entry evidence pack before GTM spend
Do not launch on a deck and a few filled shifts. Require evidence for four areas: payout logic, compliance gates, onboarding controls, and reconciliation checkpoints.
- Payout logic: idempotent execution so retries do not create duplicate payments.
- Reconciliation: payment-order audit trail showing who changed what and when.
- Compliance: documented worker-classification review and approved facility control boundaries.
- Onboarding: facility-specific orientation/training records.
The Roosevelt Institute flagged expansion risk in unfamiliar clinical environments without onboarding or facility training, based on interviews with 29 gig nurses and nursing assistants.
- Expand only after stability under real shift variability
Fill rate alone is not enough for expansion. Add gates for margin, payout exception rate, repeat-shift behavior, and quality or retention signals. AACN highlighted a case where flexible staffing improvements aligned with patient care and nurse retention, which is the direction you want before scaling. One reported deployment filled 13,000 shifts before planning expansion from 12 to 19 hospitals and nursing homes; use that as sequencing logic, not a universal benchmark.
Frequently Asked Questions
Is shift-based gig pay in healthcare actually higher than traditional staffing?
Sometimes, especially when demand spikes. Reporting on app-based nursing noted that facility-offered rates can rise with demand, so a single posted shift may be higher than some traditional staffing rates in that moment. The key differentiator is not the screenshot rate but the accepted rate for the same role, in the same market, across normal weeks as well as peak weeks.
How do surge shifts change payout volatility for platforms and workers?
Surge-linked pricing can fill hard shifts fast, but it also makes earnings and margin less predictable. When rates move up with demand, offered pay can swing by shift, which can make worker earnings and platform planning less predictable. If your fill rate only works when surge is on, treat that as a stability warning, not proof of product-market fit.
What are the biggest risks facilities face under 1099 contractor classification models?
The main risk is control mismatch, not the contract label. The IRS states that worker status depends on the substance of the relationship under common-law rules, and the Department of Labor published a new FLSA misclassification final rule on January 10, 2024, effective March 11, 2024. If a facility manages shifts, work methods, and day-to-day conduct like an employer while relying on a 1099 contractor classification label, you should expect higher scrutiny.
Which operating model is best for hospitals versus Skilled Nursing Facility (SNF) environments?
There is no universal winner. A Roosevelt Institute policy brief flagged risks from sending nurses into unfamiliar clinical environments with no onboarding or facility training, based on interviews with 29 gig nurses and nursing assistants. Model choice should be setting-specific, and wage-hour checks matter because nursing homes and residential living facilities may use overtime rules tied to 8 hours in a day or 80 hours in a 14-day period.
What evidence should founders require before entering a new market?
Ask for first-party proof that onboarding, payout traceability, and facility escalation actually work in live operations. The minimum useful pack is facility-specific onboarding records, sample reconciliation logs, and acceptance data that shows shifts clear without constant surge. One reported health-system case filled 13,000 shifts and expanded from 12 to 19 hospitals and nursing homes, but raw volume still does not replace evidence that your controls survive review.
How should teams separate verified data from vendor marketing claims?
Label each input by source type before anyone uses it in pricing or GTM: government guidance, policy brief, reported anecdote, or vendor claim. For example, messaging about delivering “reliable, cost-efficient labor at scale” is promotional copy unless you can tie it to independent evidence or your own facility data. If a claim cannot be checked against primary sources or your operating records, keep it out of margin models and legal assumptions.
Try a related tool
Researched and edited by the Gruv editorial team. Gruv builds cross-border billing, payouts, and finance-operations software for global businesses.
Sources
Includes 4 external sources outside the trusted-domain allowlist.
- dol.gov/agencies/whd/flsa/misclassification/small-en...trusted
- dol.gov/agencies/whd/workers/health-caretrusted
- irs.gov/taxtopics/tc762trusted
- irs.gov/forms-pubs/about-form-w-8-bentrusted
- aacn.org/nursing-excellence/nurse-stories/flexible-st...external
- aha.org/news/headline/2022-05-11-report-labor-costs-...external
- asrn.org/journal-advanced-practice-nursing/2934-nurse...external
- gighealth.comexternal
Educational content only. Not legal, tax, or financial advice.
Related Posts

Choosing Nursing Agency Payout Models for Shift-Based Healthcare Staffing
Choose your payout model based on operational proof, not payout-speed marketing. For healthcare staffing platforms, the real question is whether payouts stay reliable when shifts change, get canceled, or are disputed.

US Tax Reporting for Bitcoin and Ethereum Gig-Worker Payouts
If you plan to pay gig workers in Bitcoin or Ethereum, treat reporting design as part of product design from day one. Faster settlement can help operations, but weak controls can leave you with harder reconciliations and more compliance risk.

SaaS Usage-Based Pricing for Predictable Cashflow and Fewer Disputes
If you are considering **saas usage-based pricing**, treat it as an operations and collections decision first. Pricing works best when the usage unit can be measured, shown on the invoice, and explained by someone outside your product team.